Sleep Problems and Disorders
Waleed Ahmad
Mar 07, 2023
28 min read
By the end of this section, you will be able to:
Describe the symptoms and treatments of insomnia, especially sleep hygiene.
Recognize the symptoms of several parasomnias
Describe the symptoms and treatments for sleep apnea
Recognize risk factors associated with sudden infant death syndrome (SIDS) and steps to prevent it.
Describe the symptoms and treatments for narcolepsy
Many people experience disturbances in their sleep at some point in their lives. Depending on the population and sleep disorder studied, 30% to 50% population have a sleep disorder at some point in life. [1][2][3][4][5] This section will describe several sleep disorders as well as some of their treatment options.
INSOMNIA
Insomnia, a consistent difficulty falling or staying asleep, is the most common of the sleep problems; most often, it is reported as a symptom by patients with other common psychiatric disorder, especially depression or anxiety disorders. Individuals with insomnia often experience long delays when they go to bed and fall asleep. In addition, these individuals may wake up several times during the night only to find difficulty getting back to sleep. Yet, a subgroup of people experiences late insomnia or early morning waking. Late Insomnia is characteristic of severe or melancholic depression. CNX_Psych_04_04_insomniaWithDepression.png
Insomnia that occurs exclusively during the course of depression or another disorder, does not qualify the diagnostic criteria of insomnia disorder. Primary insomnia or insomnia disorder is diagnosed when it not caused by another psychiatric or medical condition, nor induced by medications or substances. The criteria for dianosing primary insomnia also requires the occurence of symptoms for at least three nights a week for at least one month [6].
It is not uncommon for people suffering from insomnia to experience anxiety about their inability to fall asleep. This becomes a self-perpetuating cycle because increased anxiety leads to increased arousal, and higher arousal levels make the prospect of falling asleep even more unlikely. Chronic insomnia is almost always associated with feeling overtired and may be associated with symptoms of depression.
Fig. 6 An illustration depicts the relationship between depression and insomnia.
Tip
Sleep-onset insomnia is more likely due to anxiety, while late-insomnia is characteristic of severe depression.
The Insomnia Severity Index (ISI) is a seven-item questionnaire that serves as a quick screening tool for insomnia. It also assesses the severity and nature of insomnia. Using a Likert-type scale, respondents are asked to rate the severity of their sleeping problems. The severity of the symptoms, the respondent’s satisfaction with his or her sleep patterns, the degree to which insomnia interferes with daily functioning, how noticeable the respondent feels their insomnia is to others, and the overall level of distress brought on by the sleep issue are all subjective aspects of the respondent’s sleep that are addressed in the questions.
Many factors may contribute to insomnia, including age, drug use, exercise, mental status, and bedtime routines. Not surprisingly, insomnia treatment may take one of several different approaches. People with insomnia might limit their use of stimulant drugs (such as caffeine) or increase their physical exercise during the day. Some people might turn to over-the-counter (OTC) or prescribed sleep medications to help them sleep, but this should be done sparingly because many sleep medications result in dependence and alter the nature of the sleep cycle, and they can increase insomnia over time. Non-pharmacological treatments are preferable. Education about the science of sleep and the implementation of sleep-hygiene techniques should always be the first step in managing insomnia.
Sleep-hygiene
The following are some of the principles of sleep hygiene. The first part would be to assess a patient’s routines based on these principles to identify maladaptive habits and tailor the recommendations accordingly. To raise the patient’s motivation to use these techniques, they may also be informed about the importance of adequate sleep and the adverse effects of long-term sleep deprivation on our mental and physical well-being.
Using consistent sleep-wake schedule even on weekends or other holidays is important; disturbance in the schedule disrupts our circadian rhythm and may lead to problems such as jet lag.
Exposure to sunlight in the day, and keeping dark at night also help regulate circadian rythms. bright light, especially blue light, inhibits melatonin production, inducing wakefulness. Thus, bright light and devices producing bright light, such as computers, tablets, and smartphones, must be avoided at night. If their use is unavoidable, brightness must be lowered to a minimum , and a blue-light blocking filter should be turned on.
Performing aerobic exercise in the morning has been shown to improve sleep at night; such a stimulating activity must, however, be avoided in the evening. The resulting sympathetic activation may lead to insomnia.
Avoiding day-time naps should be the goal; if unavoidable, a nap should occur before 3 PM and last no longer than 30 minutes.
Ideally, one specific room and bed must be used for sleep which must only be used for sleep. It must not be used for office or school work or other activities that can be performed in another room and in different settings, such as a table and a chair. This is based on the principles of classical conditioning. Over time, as the bed is used specifically for sleep, it becomes a conditioned stimulus and elicits sleep.
Foods containing caffeine, such as tea, coffee, energy drinks, and cola drinks, must be avoided after 4 PM. Similarly, excessive consumption of sweets, smoking cigarette, or using alcohol may impair sleep. Tryptophan containing foods, such as milk, is encouraged; it is a precursor of serotonin and melatonin and helps with sleep. The quantity of food consumed should be enough to avoid discomfort due to an empty stomach or overeating. A meal should be taken at least a couple of hours before bedtime.
For some, sleep restriction may be helpful. In this, the patient is enquired about the approximate sleep duration, and their bedtime is restricted only to that much interval. For example, suppose a patient usually falls asleep at 1:00 AM after spending several hours in their bed. In that case, they must go to bed at around 1 AM and leave immediately upon awakening. This technique is also based on conditioning, as discussed above. Gradually, bedtime duration increases as the patient’s sleep improve.
In stimulus control, the patient must avoid going to their bed until they feel drowsy. This interval should be spent sitting in a calm, dark environment and a comfortable chair. Using earbuds with a masking effect can help block noise from a source that can be controlled. White noise machines may also help, especially for those with tinnitus.
Discussing or thinking about distressing or exciting issues can cause sympathetic responses and impair sleep. If issues must be discussed, they should be discussed in the daytime, long before the time for sleep. To avoid preoccupation with intrusive thoughts, the patient is advised to count backward from 500.
During bedtime, room temperature should be at a level where one would need a light blanket. People more readily fall asleep when the temperature is low or when their body temperature drops. A warm water bath before bedtime can thus help induce sleep.
Repeatedly checking time and actively trying to fall asleep is similarly distressing and prevents one from falling asleep. Instead, the patient is advised to try to stay awake.
If anxiety is significant, regular progressive muscle relaxation before bedtime will help.
Aromatherapy with lavender oil may also help.
Cognitive-behavioral therapy for insomnia (CBT-I), is the first-line high-intensity therapy and is preferable to the use of hypnotics. Behaviours that could contribute to insomnia (e.g., spending more waking time in bed) are identified and eliminated or replaced. Implementation of sleep hygiene techniques is an integral component of CBT-I. The treatment also includes stress management techniques. Other components are sleep-restriction and stimulus control. Cognitive-behavioral therapy has been shown effective to treat insomnia. [7][8]
Sleep Disruption in Depression
In patients with depression, there is a disturbance of sleep continuity; they spend more time awake and have increased sleep fragmentation. Early morning wakening occurs characteristically in severe and melancholic depression.
Evidence has shown a disturbance in the sleep architecture, with decreased slow-wave sleep on electroencephalography.
Disturbances in REM sleep include shortened REM latency, more REM activity (higher percentage) in the first ½ of the night and a higher REM density. Sleep deprivation (especially deprivation of REM sleep) has shown a temporary but beneficial effect on mood in depressed patients resulting in quick improvement. Antidepressants impair REM sleep; there is a rebound of REM sleep on discontinuation.
PARASOMNIAS
Parasomnias comprise a group of sleep disorders in which unwanted, disruptive motor activity or experiences during sleep play a role. Parasomnias can occur in either REM or NREM phases of sleep. Sleepwalking, restless leg syndrome, and night terrors are all examples of parasomnias (Mahowald & Schenck, 2000).
Sleepwalking
In sleepwalking, or somnambulism, the sleeper engages in relatively complex behaviors ranging from wandering about to driving an automobile. During a sleepwalking episode, sleepers often have their eyes open but are not responsive to attempts to communicate with them. Sleepwalking most often occurs during slow-wave sleep, but it can occur at any time during a sleep period in some affected individuals. [9]
Historically, somnambulism has been treated with various pharmacotherapies ranging from benzodiazepines to antidepressants. However, the success rate of such treatments is questionable. Guilleminault et al. (2005) [10] found that sleepwalking was not alleviated with benzodiazepines. However, all of their somnambulistic patients who also suffered from sleep-related breathing problems showed a marked decrease in sleepwalking when their breathing problems were effectively treated.
Environmental Approaches to Manage Sleepwalking
The aim of these is mainly to prevent harm and, if possible, prevent the episodes from occurring.
Reassure parents about its benign nature.
Identify and avoid precipitating factors
Avoid waking the patient up during the episode.
Remove obstructions in the bedroom and items on which they may stumble and fall.
Secure windows and cover windows with heavy curtains.
Install locks or alarms on outside doors
Use a nightlight in case
Sleep on the ground floor and place barriers in stairways so to prevent them from the rooftop
Scheduled awakenings (15-30 minutes prior) may be helpful if the episodes occur consistently at roughly the same time.
Forensic Implications: Sleepwalking as a Court Defense?
On January 16, 1997, Scott Falater sat down to dinner with his wife and children and told them about difficulties he was experiencing on a project at work. After dinner, he prepared some materials to lead a church youth group the following morning. Then he attempted to repair the family’s swimming pool pump before retiring to bed. The following morning, he awoke to barking dogs and unfamiliar voices from downstairs. As he went to investigate what was going on, he was met by a group of police officers who arrested him for the murder of his wife. [11]
Yarmila Falater’s body was found in the family’s pool with 44 stab wounds. A neighbor called the police after witnessing Falater standing over his wife’s body before dragging her into the pool. Upon a search of the premises, police found blood-stained clothes and a bloody knife in the trunk of Falater’s car, and he had blood stains on his neck.
Remarkably, Falater insisted that he had no recollection of hurting his wife in any way. His children and his wife’s parents all agreed that Falater had an excellent relationship with his wife, and they could not think of a reason that would provide any motive to murder her. [11]
Scott Falater had a history of regular episodes of sleepwalking as a child and he had even behaved violently toward his sister once when she tried to prevent him from leaving their home in his pajamas during a sleepwalking episode. He suffered from no apparent anatomical brain anomalies or psychological disorders. It appeared that Scott Falater had killed his wife in his sleep, or at least, that is the defense he used when he was trialed for his wife’s murder. [11]
In Falater’s case, a jury found him guilty of first-degree murder in June of 1999 (CNN, 1999); however, there are other murder cases where the sleepwalking defense has been used successfully. As scary as it sounds, many sleep researchers believe that homicidal sleepwalking is possible in individuals suffering from the types of sleep disorders described below (Broughton et al., 1994; Cartwright, 2004; Mahowald, Schenck, & Cramer Bornemann, 2005; Pressman, 2007).
REM Sleep Behaviour Disorder (RBD)
REM sleep behavior disorder (RBD) occurs when the muscle paralysis associated with the REM sleep phase does not occur. Individuals who suffer from RBD have high physical activity levels during REM sleep, especially during disturbing dreams. These behaviours vary widely, including kicking, punching, scratching, yelling, and behaving like an animal that has been frightened or attacked. People who suffer from this disorder can injure themselves or their sleeping partners when engaging in these behaviors. Furthermore, these types of behaviours ultimately disrupt sleep, although affected individuals have no memories that these behaviors have occurred. [12]
Risk of Harm in RBD
Patients with RBD may exhibit violent behaviours and cause injury to themselves or others. Environmental modification and education of the family about the risks and ways of prevention is important part of the treatment.
This disorder is associated with several neurodegenerative diseases, such as Parkinson’s. This relationship is so robust that some view the presence of RBD as a potential aid in diagnosing and treating several neurodegenerative diseases. [13] Clonazepam, is most often used to treat RBD. It is administered alone or in conjunction with doses of melatonin (the hormone secreted by the pineal gland). As part of treatment, the sleeping environment is often modified to make it safer for those suffering from RBD. [14]
Other Parasomnias
A person with restless leg syndrome has uncomfortable sensations in the legs during periods of inactivity or when trying to fall asleep. This discomfort is relieved by deliberately moving the legs, which, not surprisingly, contributes to difficulty in falling or staying asleep. Restless leg syndrome is quite common and has been associated with several other medical diagnoses, such as chronic kidney disease and diabetes [15] (Mahowald & Schenck, 2000). There are a variety of drugs that treat restless leg syndrome: benzodiazepines, opiates, and anticonvulsants (Restless Legs Syndrome Foundation, n.d.).
Night terrors present as a panic in the sufferer and are often accompanied by screams and attempts to escape from the immediate environment (Mahowald & Schenck, 2000). Although individuals suffering from night terrors appear to be awake, they generally have no memories of the events, and attempts to console them are ineffective. Typically, individuals suffering from night terrors will fall back asleep again within a short time. Night terrors occur during the NREM phase of sleep (Provini, Tinuper, Bisulli, & Lagaresi, 2011). Generally, treatment for night terrors is unnecessary unless there is some underlying medical or psychological condition that is contributing to the night terrors (Mayo Clinic, n.d.).
SLEEP APNOEA
Sleep apnea is defined by episodes during which a sleeper’s breathing stops. These episodes can last 10–20 seconds or longer and often are associated with brief periods of arousal. While individuals suffering from sleep apnea may not be aware of these repeated sleep disruptions, they experience increased fatigue levels. Many individuals diagnosed with sleep apnea first seek treatment because their sleeping partners indicate that they snore loudly and stop breathing for extended periods while sleeping. [16]
Presentation of Sleep Apnoea
Individuals with sleep apnoea are unaware of their sleep disruptions. Fatigue, excessive daytime sleepiness, and, if a partner has obersved, snoring are important indicators.
Sleep apnea is much more common among obese people and is often associated with loud snoring. Surprisingly, sleep apnea may exacerbate cardiovascular disease. [17] While sleep apnea is less common in thin people, a person who snores loudly or gasps for air should be evaluated for sleep apnea regardless of weight.
While people are often unaware of their sleep apnea, they are keenly aware of some of the adverse consequences of insufficient sleep. Consider a patient who believed that as a result of his sleep apnea, he:
“had three car accidents in six weeks. They were ALL my fault. Two of them I did not even know I was involved in until afterward.”
– Henry & Rosenthal, 2013, p. 52.
It is not uncommon for people suffering from undiagnosed or untreated sleep apnea to fear that their careers will be affected by the lack of sleep, illustrated by this statement from another patient,
“I am in a job where there is a premium on being mentally alert. I was sleepy… and having trouble concentrating…. It was getting to the point where it was kind of scary”
– Henry & Rosenthal, 2013, p. 52 [16]
The following are the clinical features of sleep apnoea:
Loud snoring (95%)
Daytime sleepiness (90%)
Unrefreshed or disturbed sleep
Morning headache and confusion
Nocturnal choking
Enuresis
Swelling of the ankles
There are two types of sleep apnea: obstructive sleep apnea and central sleep apnea. Obstructive sleep apnea occurs when an individual’s airway becomes blocked during sleep, and the air is prevented from entering the lungs. In central sleep apnea, disruption in signals sent from the brain that regulate breathing cause periods of interrupted breathing (White, 2005).
One of the most common sleep apnea treatments involves using continuous positive airway pressure (CPAP) device. It includes a mask that fits over the sleeper’s nose and mouth, which is connected to a pump that pumps air into the person’s airways, forcing them to remain open, as shown in [fig. %s) <cnx_psych_04_04_cpap>. Some newer CPAP masks are smaller and cover only the nose. This treatment option has proven effective for people suffering from mild to severe cases of sleep apnea. [18] However, alternative treatment options are being explored because consistent compliance by users of CPAP devices is a problem. Recently, a new EPAP (expiratory positive air pressure) device has shown promise in double-blind trials as one su.ch alternative. [19]
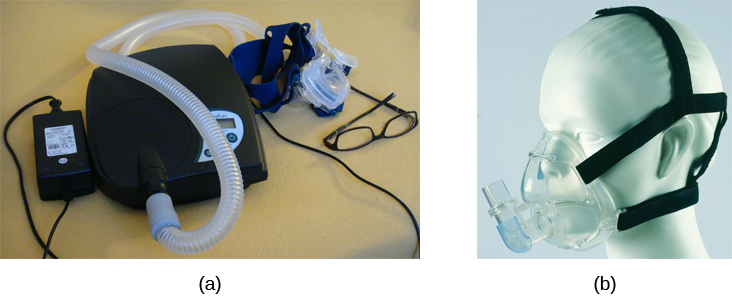
Fig. 7 Photograph A shows a CPAP device. Photograph B shows a clear full-face CPAP mask attached to a mannequin’s head with straps
Benzodiazepines and CNS depressants are contraindicated in OSA.
These medications, espeically when used in combination, may cause respiratory depression.
SIDS
In sudden infant death syndrome (SIDS) an infant stops breathing during sleep and dies. Infants younger than 12 months appear to be at the highest risk for SIDS, and boys have a greater risk than girls. Several risk factors have been associated with SIDS including premature birth, smoking within the home, and hyperthermia. There may also be differences in both brain structure and function in infants that die from SIDS [20][21] (Thach, 2005).
Preventing SIDS
The substantial amount of research on SIDS has led to several recommendations to parents to protect their children ([link]). For one, research suggests that:
Infants should be placed on their backs when put down to sleep, and
Their cribs should not contain items that pose suffocation threats, such as blankets, pillows or padded crib bumpers (cushions that cover the crib bars).
Infants should not have caps placed on their heads when put down to sleep in order to prevent overheating, and
People in the child’s household should abstain from smoking in the home.
Recommendations like these have helped to decrease the number of infant deaths from SIDS in recent years [22][23]

Fig. 8 The “Safe to Sleep” campaign logo shows a baby sleeping and the words “safe to sleep.”
Safe to Sleep campaign started in 1994 as Back to Sleep to teach people about reducing the risk of SIDS.
Excessive Daytime Sleepiness
Excessive daytime sleepiness (EDS) may occur due to primary hypersomnia, sleep deprivation, or sleep disorder. The following is a summary of common causes of EDS.
Aetiology
Insufficient night-time sleep a. Unsatisfactory irregular sleep routines b. Circadian rhythm sleep disorders c. Frequent parasomnias d. Chronic physical illness e. Psychiatric disorders
Pathological sleep a. Obstructive sleep apnoea b. Narcolepsy c. Other CNS disease d. Drug effects e. Kleine-Levin syndrome f. Atypical depressive illness
Epworth Sleepiness Scale (ESS) is a self-rated scale used by clinicians to assess daytime sleepiness. The scale contains a total of 8 items, and each scored 0-3. From a total score of 24, 11 suggest some degree of daytime sleepiness, while 16 suggest excessive daytime sleepiness.
The Multiple Sleep Latency Test (MSLT) is a tool determines whether a person has physical fatigue or actual excessive daytime sleepiness, and to test for central diseases of hypersomnolence such narcolepsy or idiopathic hypersomnia. It measures the sleep-latency, ie, the interval between the beginning of a daytime nap and the onset of the first indications of sleep. The test’s premise is that people fall asleep more quickly when they are more sleepy. Following an overnight sleep-study, the procedure is performed comprising four or five 20-minute nap opportunities spaced two hours apart. The patient’s brain waves, EEG, muscle activity, and eye movements are monitored and recorded during the test. The entire procedure typically lasts a day and takes around 7 hours. Multiple opportunities ascertain whether there are irregularities in duration of sleep-latency.
NARCOLEPSY
Unlike the other sleep disorders described in this section, a person with narcolepsy cannot resist falling asleep at inopportune times. These sleep episodes are often associated with cataplexy, a loss of muscle tone, often triggerd by extreme emotions cuasing muscle weakness, which in some cases involve, complete paralysis of the voluntary muscles. This is similar to the kind of paralysis experienced by healthy individuals during REM sleep. [24][25][26] Narcoleptic episodes take on other features of REM sleep. For example, around one-third of individuals diagnosed with narcolepsy experience vivid, dream-like hallucinations during narcoleptic attacks. [27]
Surprisingly, narcoleptic episodes are often triggered by states of heightened arousal or stress. The typical episode can last from a minute or two to half an hour. Once awakened from a narcoleptic attack, people report that they feel refreshed. [28]
Frequent narcoleptic episodes may interfere with the ability to perform one’s job or complete schoolwork, and in some situations, narcolepsy can result in significant harm and injury (e.g., driving a car or operating machinery or other potentially dangerous equipment).
In addition to these episodes, patients with narcolpey may experience excessive daytime sleepiness.
Symptoms not associated with a narcoleptic episode include sleep paralysis and hypnagogic hallucinations. Sleep paralysis is a transient and generalized inability to move or speak during the transition between sleep and wakefulness, typically occur while falling asleep. The paralysis is flaccid, and usually complete. Episodes of sleep paralysis usually last only a few seconds, and less than one minute. Hypnagogic hallucinations also occur when the individual is about to fall asleep.
Patients with narcolepsy have a reduced sleep latency during the day and greatly reduced REM latency at night; the patient may enter REM stage at sleep onset.
Generally, narcolepsy is treated using psychomotor stimulant drugs, such as amphetamines. [29] These drugs promote increased levels of neural activity. Narcolepsy is associated with reduced levels of the signaling molecule hypocretin in some areas of the brain (De la Herrán-Arita & Drucker-Colín, 2012; Han, 2012), and the traditional stimulant drugs do not directly affect this system. Therefore, it is quite likely that new medications that are developed to treat narcolepsy will be designed to target the hypocretin system.
Variability of Presentation in Narcolepsy
There is tremendous variability among sufferers regarding how symptoms of narcolepsy manifest and the effectiveness of currently available treatment options. This is illustrated by McCarty’s case study (2010) [30] of a 50-year-old woman who sought help for the excessive sleepiness during regular waking hours that she had experienced for several years. She indicated that she had fallen asleep at inappropriate or dangerous times, including eating, socializing with friends, and driving her car. During periods of emotional arousal, the woman complained that she felt some weakness in the right side of her body. Although she did not experience any dream-like hallucinations, she was diagnosed with narcolepsy due to sleep testing. The fact that her cataplexy occurred solely on the right side of her body was quite unusual. Early attempts to treat her condition with a stimulant drug alone were unsuccessful. However, her condition improved dramatically with a combination of a stimulant drug and an antidepressant.
Kleine-Levin Syndrome
The Kleine-Levin syndrome is a rare secondary sleep disorder. Most cases are in young men with onset in early adolescence Patients experience episodes of somnolence and hyperphagia, often lasting days or weeks and with long intervals of normality between them.
Patients can always be aroused from the daytime sleep, but are irritable and occasionally exhibit aggression on waking. Usually, the patient only wakes to eat or empty bladder and bowels during an episode. Incontinence does not occur. When awake, he eats voraciously, typically eating any food in sight, although the patient rarely complains of hunger.
Mental symptoms: Some are muddled and experience depression, and disorientation. Vivid imagery may be prominent, with waking fantasies which are difficult to disentangle from vivid dreams Visual and auditory hallucinations may also occur. Hypersexuality occurs in around 25 % of cases.
Physical signs are few and less frequent. Pulse and temperature is usually normal. Pupils may be unequal and plantar reflexes may be upgoing. EEG shows the usual changes of drowsiness or sleep.
Atypical depression vs Klein-Levin Syndrome.
Notice the overlap of symptoms between atypical depression and KLS. Patients with KLS may exhibit irritablity and depression. Likewise, pateints with atypical depression may experience overeating and oversleeping.
What would help us to differentiate the two?
Psychiatric Disorders and Sleep Architecture
- Depression
reduced duration of stages 3 and 4
reduced REM latency
REM occurs earlier in the night
- Schizophrenia
reduced slow-wave sleep
reduced REM
- Anxiety
increased duration of stages 1 and 2
reduced efficacy of sleep
- Panic disorder
increased sleep latency
- Alcoholism
increased delta
increased REM sleep
increased alpha activity
- Alzheimer’s disease
increased sleep
fragmentation
reduced sleep efficiency
The Effects of Drugs on Sleep
Alcohol has a biphasic action on sleep. In the first half of the night, it decreases sleep onset latency (promotes sleep initially). Regarding sleep architecture, it leads to an increase in the duration of deep sleep and relative deprivation of REM sleep. In the night’s second half, there is a rebound increase in REM sleep duration. The sleep promotion associated with small doses of alcohol may be related to prior sleep deprivation. Alcohol also exacerbates sleep-related breathing disorders, sleep apnoea, and sleepwalking. Chronic use of excessive amounts of alcohol disrupts all stages of sleep. During withdrawal, the total sleep time is reduced and non-REM sleep is particularly affected.
Drug |
Total Sleep time |
REM |
Light sleep Stages 1 & 2 |
Deep sleep Stages 3 & 4 |
|---|---|---|---|---|
Opioids |
↓ |
↓ |
↓ |
↓ |
Caffeine |
↓ |
↓ REM latency ↑ REM sleep |
slightly ↓ |
|
Am phetamines, cocaine |
initial insomnia and reduced TST |
↑ REM latency ↓ REM sleep |
Summary
Many individuals suffer from some sleep disorder or disturbance at some point. Insomnia is a common experience in which people have difficulty falling or staying asleep. Parasomnias involve unwanted motor behavior or experiences throughout the sleep cycle, including RBD, sleepwalking, restless leg syndrome, and night terrors. Sleep apnea occurs when individuals stop breathing during sleep; in the case of sudden infant death syndrome, infants will stop breathing during sleep and die. Narcolepsy involves an irresistible urge to fall asleep during waking hours and is often associated with cataplexy and hallucination.
QuestionThe loss of muscle tone or control that is often associated with narcolepsy:
RBD
CPAP
cataplexy
insomnia
Check Answer
C
An individual may suffer from ________ if there is a disruption in the brain signals that are sent to the muscles that regulate breathing.
central sleep apnea
obstructive sleep apnea
narcolepsy
SIDS
Check Answer
A
The most common treatment for ________ involves the use of amphetamine-like medications.
sleep apnea
RBD
SIDS
narcolepsy
Check Answer
D
________ is another word for sleepwalking.
insomnia
somnambulism
cataplexy
narcolepsy
B
Critical Thinking Questions
One of the recommendations that therapists will make to people with insomnia is to spend less waking time in bed. Why do you think spending waking time in bed might interfere with the ability to fall asleep later?
Answers will vary. One possible explanation might invoke principles of associative learning. If the bed represents a place for socializing, studying, eating, and so on, then it is possible that it will become a place that elicits higher levels of arousal, which would make falling asleep at the appropriate time more difficult. Answers could also consider a self-perpetuating cycle referred to when describing insomnia. If an individual is having trouble falling asleep and that generates anxiety, it might make sense to remove him from the context where sleep would normally take place to try to avoid anxiety being associated with that context.
How is narcolepsy with cataplexy similar to and different from REM sleep?
Similarities include muscle atony and the hypnagogic hallucinations associated with narcoleptic episodes. The differences involve the uncontrollable nature of narcoleptic attacks and the fact that these come on in situations that would typically not be associated with sleep of any kind (e.g., instances of heightened arousal or emotionality).
Personal Application Question
What factors might contribute to your own experiences with insomnia?
Glossary
- cataplexy
lack of muscle tone or muscle weakness, and in some cases, complete paralysis of the voluntary muscles
- central sleep apnea
sleep disorder with periods of interrupted breathing due to a disruption in signals sent from the brain that regulate breathing ^
- cognitive-behavioral therapy
psychotherapy that focuses on cognitive processes and problem behaviors that is sometimes used to treat sleep disorders such as insomnia
- continuous positive airway pressure (CPAP)
device used to treat sleep apnea; includes a mask that fits over the sleeper’s nose and mouth, which is connected to a pump that pumps air into the person’s airways, forcing them to remain open ^
- narcolepsy
sleep disorder in which the sufferer cannot resist falling to sleep at inopportune times ^
- night terror
sleep disorder in which the sleeper experiences a sense of panic and may scream or attempt to escape from the immediate environment
- obstructive sleep apnea
sleep disorder defined by episodes when breathing stops during sleep as a result of blockage of the airway ^
- parinsomnia
one of a group of sleep disorders characterized by unwanted, disruptive motor activity and/or experiences during sleep ^
- REM sleep behavior disorder (RBD)
sleep disorder in which the muscle paralysis associated with the REM sleep phase does not occur; sleepers have high levels of physical activity during REM sleep, especially during disturbing dreams ^
- restless leg syndrome
sleep disorder in which the sufferer has uncomfortable sensations in the legs when trying to fall asleep that are relieved by moving the legs ^
- sleep apnea
sleep disorder defined by episodes during which breathing stops during sleep ^
- sleepwalking
(also, somnambulism) sleep disorder in which the sleeper engages in relatively complex behaviors
- sudden infant death syndrome (SIDS)
infant (one year old or younger) with no apparent medical condition suddenly dies during sleep
References
Copyright Notice
This work is (being) adapted from on OpenStax Psychology 2e which is licensed under creative commons attribution 4.0 license. We license our work under a similar license. If you copy, adapt, remix or build up on work, you must give appropriate credit, provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use.